
Dislocated shoulder
| Dislocated shoulder | |
|---|---|
 | |
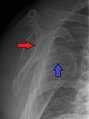
| Anterior dislocation of the left shoulder. | |
| Specialty | Emergency medicine, orthopedics |
| Symptoms | Shoulder pain |
| Complications | Bankart lesion, Hill-Sachs lesion, rotator cuff tear, axillary nerve injury[1] |
| Types | Anterior, posterior, inferior, superior[2][1] |
| Causes | Fall onto an outstretched arm or the shoulder.[3] |
| Diagnostic method | Based on symptoms, X-rays[2] |
| Treatment | Shoulder reduction, arm sling[1][2] |
| Medication | Procedural sedation and analgesia, intraarticular lidocaine[4] |
| Prognosis | Recurrence common in young people[3] |
| Frequency | 24 per 100,000 per year (US)[1] |

A dislocated shoulder is a condition in which the head of the humerus is detached from the glenoid fossa.[2] Symptoms include shoulder pain and instability.[2] Complications may include a Bankart lesion, Hill-Sachs lesion, rotator cuff tear, or injury to the axillary nerve.[1]
A shoulder dislocation often occurs as a result of a fall onto an outstretched arm or onto the shoulder.[3] Diagnosis is typically based on symptoms and confirmed by X-rays.[2] They are classified as anterior, posterior, inferior, and superior with most being anterior.[2][1]
Treatment is by shoulder reduction which may be accomplished by a number of techniques.[1] These include traction-countertraction, external rotation, scapular manipulation, and the Stimson technique.[1] After reduction X-rays are recommended for verification.[1] The arm may then be placed in a sling for a few weeks.[2] Surgery may be recommended in those with recurrent dislocations.[2]
Not all patients require surgery following a shoulder dislocation. There is moderate quality evidence that patients who receive physical therapy after an acute shoulder dislocation will not experience recurrent dislocations.[5] It has been shown that patients who do not receive surgery after a shoulder dislocation do not experience recurrent dislocations within two years of the initial injury.[5]
About 1.7% of people have a shoulder dislocation within their lifetime.[3] In the United States this is about 24 per 100,000 people per year.[1] They make up about half of major joint dislocations seen in emergency departments.[1] Males are affected more often than females.[1] Most shoulder dislocations occur as a result of sports injuries.[5]
Signs and symptoms
[edit]- Significant pain, sometimes felt along the arm past the shoulder.
- Sensation that the shoulder is slipping out of the joint during abduction and external rotation.[6]
- Shoulder and arm held in external rotation (anterior dislocation), or adduction and internal rotation (posterior dislocation).[6] Resistance of all movement.
- Numbness of the arm.
- Visibly displaced shoulder. Some dislocations result in the shoulder appearing unusually square.
- No palpable bone on the side of the shoulder.
Diagnosis
[edit]A diagnosis of shoulder dislocation is often suspected based on the person's history and physical examination. Radiographs are made to confirm the diagnosis. Most dislocations are apparent on radiographs showing incongruence of the glenohumeral joint. Posterior dislocations may be hard to detect on standard AP radiographs, but are more readily detected on other views. After reduction, radiographs are usually repeated to confirm successful reduction and to detect bone damage. After repeated shoulder dislocations, an MRI scan may be used to assess soft tissue damage. In regards to recurrent dislocations, the apprehension test (anterior instability) and sulcus sign (inferior instability) are useful methods for determining predisposition to future dislocation.[citation needed]
There are three main types of dislocations: anterior, posterior, and inferior.[7]
Anterior (forward)
[edit]
In over 95% of shoulder dislocations, the humerus is displaced anteriorly.[8] In most of those, the head of the humerus comes to rest under the coracoid process, referred to as sub-coracoid dislocation. Sub-glenoid, subclavicular, and, very rarely, intrathoracic or retroperitoneal dislocations may also occur.[9]
Anterior dislocations are usually caused by a direct blow to, or fall on, an outstretched arm. The person typically holds his/her arm externally rotated and slightly abducted.[10]
A Hill–Sachs lesion is an impaction of the head of the humerus left by the glenoid rim during dislocation.[6] Hill-Sachs deformities occur in 35–40% of anterior dislocations. They can be seen on a front-facing X-ray when the arm is in internal rotation.[11] Bankart lesions are disruptions of the glenoid labrum with or without an avulsion of bone fragment.[12]
Damage to the axillary artery[13] and axillary nerve (C5, C6) may result. The axillary nerve is injured in 37% making it the most commonly injured structure with this type of injury.[14] Other common, associated, nerve injuries include injury to the suprascapular nerve (29%) and the radial nerve (22%).[14] Axillary nerve damage results in a weakened or paralyzed deltoid muscle and as the deltoid atrophies unilaterally, the normal rounded contour of the shoulder is lost. A person with injury to the axillary nerve will have difficulty in abducting the arm from approximately 15° away from the body. The supraspinatus muscle initiates abduction from a fully adducted position.[citation needed]
-
 An anterior dislocation of the shoulder
An anterior dislocation of the shoulder -
 Anterior dislocation of the right shoulder. AP X ray
Anterior dislocation of the right shoulder. AP X ray -
 Anterior dislocation of the right shoulder. Y view X ray.
Anterior dislocation of the right shoulder. Y view X ray.



Posterior (backward)
[edit]
Posterior dislocations are uncommon, and are typically due to the muscle contraction from electric shock or seizure.[6] They may be caused by strength imbalance of the rotator cuff muscles. People with dislocated shoulders typically present holding their arm internally rotated and adducted, and exhibiting flattening of the anterior shoulder with a prominent coracoid process.[citation needed]
Posterior dislocations may go unrecognized, especially in an elderly person[15] and in people who are in the state of unconscious trauma.[16] An average interval of 1 year was noted between injury and diagnosis in a series of 40 people.[17]
Inferior (downward)
[edit]
Inferior dislocation is the least likely, occurring in less than 1%. This condition is also called luxatio erecta because the arm appears to be permanently held upward or behind the head.[18] It is caused by a hyper abduction of the arm that forces the humeral head against the acromion.[19] Such injuries have a high complication rate as many vascular, neurological, tendon, and ligament injuries are likely to occur from this mechanism of injury.
Treatment
[edit]Prompt medical treatment should be sought for suspected dislocation. Usually, the shoulder is kept in its current position by use of a splint or sling. A pillow between the arm and torso may provide support and increase comfort. Strong analgesics are needed to allay the pain of a dislocation and the distress associated with it.[citation needed]
Reduction
[edit]
Shoulder reduction may be accomplished with a number of techniques including traction-countertraction, external rotation, scapular manipulation, Stimson technique, Cunningham technique, or Milch technique.[1][3] Pain can be managed during the procedures either by procedural sedation and analgesia or injected lidocaine into the shoulder joint.[20] Injecting lidocaine into the joint may be less expensive and faster.[4] If a shoulder cannot be relocated in the emergency room, relocation in the operating room may be required.[1] This situation occurs in about 7% of cases.[1]
[21] Stimson procedure is the least painful, widely used shoulder reduction technique. In this procedure a weight is attached to the wrist while the injured arm is hanging off an examination table for between 20 and 30 minutes. The arm is then slowly rotated until the shoulder is relocated. Sedatives are used in Stimson procedure and first time Stimson reduction for acute shoulder dislocation requires wearing arm slings for between 2 and 4 weeks.
Post-reduction
[edit]There is no strong evidence of a difference in outcomes when the arm is immobilized in internal versus external rotation following an anterior shoulder dislocation.[22][23] A 2008 study of 300 people for almost six years found that conventional shoulder immobilisation in a sling offered no benefit.[24]
Surgery
[edit]
In young adults engaged in highly demanding activities shoulder surgery may be considered.[25] Arthroscopic surgery techniques may be used to repair the glenoidal labrum, capsular ligaments, biceps long head anchor or SLAP lesion or to tighten the shoulder capsule.[26]
Arthroscopic stabilization surgery has evolved from the Bankart repair, a time-honored surgical treatment for recurrent anterior instability of the shoulder.[27] However, the failure rate following Bankart repair has been shown to increase markedly in people with significant bone loss from the glenoid (socket).[28] In such cases, improved results have been reported with some form of bone augmentation of the glenoid such as the Latarjet operation.[29][30][31]
Although posterior dislocation is much less common, instability following it is no less challenging and, again, some form of bone augmentation may be required to control instability.[32] Damaged ligaments, including labral tears, occurring as a result of posterior dislocations may be treated arthroscopically.[citation needed]
There remains those situations characterized by multidirectional instability, which have failed to respond satisfactorily to rehabilitation, falling under the AMBRI classification previously noted. This is usually due to an overstretched and redundant capsule which no longer offers stability or support. Traditionally, this has responded well to a 'reefing' procedure known as an open inferior capsular shift.[33] More recently, the procedure has been carried out as an arthroscopic procedure, rather than open surgery, again with comparable results.[33] Most recently, the procedure has been carried out using radio frequency technology to shrink the redundant shoulder capsule (thermal capsular shrinkage);[34] while long-term results of this development are currently unproven, recent studies show thermal capsular shrinkage have higher failure rates with the highest number of cases of instability recurrence and re-operation.[31]
Physiotherapy
[edit]Following shoulder reduction, most people are given self-management advice on recovery, such as home exercises, but some receive additional physiotherapy. A randomised controlled trial showed similar shoulder function after 6 months between those who received self-management advice only and those who had extra physiotherapy. Both groups also had a similar number of complications.[35][36]
Prognosis
[edit]After an anterior shoulder dislocation, the risk of a future dislocation is about 20%. This risk is greater in males than females.[37]
See also
[edit]References
[edit]- ^ a b c d e f g h i j k l m n o Bonz J, Tinloy B (May 2015). "Emergency department evaluation and treatment of the shoulder and humerus". Emergency Medicine Clinics of North America. 33 (2): 297–310. doi:10.1016/j.emc.2014.12.004. PMID 25892723.
- ^ a b c d e f g h i "Dislocated Shoulder". OrthoInfo - AAOS. October 2007. Archived from the original on 17 June 2017. Retrieved 13 October 2017.
- ^ a b c d e Cunningham NJ (2005). "Techniques for reduction of anteroinferior shoulder dislocation". Emergency Medicine Australasia. 17 (5–6): 463–71. doi:10.1111/j.1742-6723.2005.00778.x. PMID 16302939. S2CID 18146330.
- ^ a b Wakai A, O'Sullivan R, McCabe A (April 2011). "Intra-articular lignocaine versus intravenous analgesia with or without sedation for manual reduction of acute anterior shoulder dislocation in adults". The Cochrane Database of Systematic Reviews. 2013 (4): CD004919. doi:10.1002/14651858.CD004919.pub2. PMC 8859829. PMID 21491392.
- ^ a b c Kavaja L, Lähdeoja T, Malmivaara A, Paavola M (December 2018). "Treatment after traumatic shoulder dislocation: a systematic review with a network meta-analysis". British Journal of Sports Medicine. 52 (23): 1498–1506. doi:10.1136/bjsports-2017-098539. PMC 6241619. PMID 29936432.
- ^ a b c d Essentials of musculoskeletal care. Sarwark, John F. Rosemont, Ill.: American Academy of Orthopaedic Surgeons. 2010. ISBN 978-0892035793. OCLC 706805938.
{{cite book}}: CS1 maint: others (link) - ^ "Shoulder Dislocations Overview". StatPearls. StatPearls. 2024. PMID 29083735.
- ^ Rabow MW, McPhee SJ, Papadakis MA (2017-09-02). Current medical diagnosis & treatment 2018. Papadakis, Maxine A., McPhee, Stephen J., Rabow, Michael W. (Fifty-seventh ed.). New York. ISBN 9781259861482. OCLC 959649794.
{{cite book}}: CS1 maint: location missing publisher (link) - ^ Shoulder Dislocations at eMedicine
- ^ "Shoulder Dislocations Overview". StatPearls. StatPearls. 2024. PMID 29083735.
- ^ Riebel GD, McCabe JB (March 1991). "Anterior shoulder dislocation: a review of reduction techniques". The American Journal of Emergency Medicine. 9 (2): 180–8. doi:10.1016/0735-6757(91)90187-o. PMID 1994950.
- ^ "Shoulder Dislocations Overview". StatPearls. StatPearls. 2024. PMID 29083735.
- ^ Kelley SP, Hinsche AF, Hossain JF (November 2004). "Axillary artery transection following anterior shoulder dislocation: classical presentation and current concepts". Injury. 35 (11): 1128–32. doi:10.1016/j.injury.2003.08.009. PMID 15488503.
- ^ a b Malik S, Chiampas G, Leonard H (November 2010). "Emergent evaluation of injuries to the shoulder, clavicle, and humerus". Emergency Medicine Clinics of North America. 28 (4): 739–63. doi:10.1016/j.emc.2010.06.006. PMID 20971390.
- ^ Dislocations, Shoulder at eMedicine
- ^ Life in the Fast Lane Posterior Shoulder Dislocation Archived January 6, 2010, at the Wayback Machine
- ^ Hawkins RJ, Neer CS, Pianta RM, Mendoza FX (January 1987). "Locked posterior dislocation of the shoulder". The Journal of Bone and Joint Surgery. American Volume. 69 (1): 9–18. doi:10.2106/00004623-198769010-00003. PMID 3805075. Archived from the original on 2007-10-13.
- ^ Dislocations, Shoulder~clinical at eMedicine
- ^ Yamamoto T, Yoshiya S, Kurosaka M, Nagira K, Nabeshima Y (December 2003). "Luxatio erecta (inferior dislocation of the shoulder): a report of 5 cases and a review of the literature". American Journal of Orthopedics. 32 (12): 601–3. PMID 14713067.
- ^ Fitch RW, Kuhn JE (August 2008). "Intraarticular lidocaine versus intravenous procedural sedation with narcotics and benzodiazepines for reduction of the dislocated shoulder: a systematic review". Academic Emergency Medicine. 15 (8): 703–8. doi:10.1111/j.1553-2712.2008.00164.x. PMID 18783486.
- ^ "Medically Sound: A Bump to a Shoulder – Dislocated, Fractured". Medically Sound. 2020-09-14. Retrieved 2020-11-01.
- ^ Whelan DB, Kletke SN, Schemitsch G, Chahal J (February 2016). "Immobilization in External Rotation Versus Internal Rotation After Primary Anterior Shoulder Dislocation: A Meta-analysis of Randomized Controlled Trials". The American Journal of Sports Medicine. 44 (2): 521–32. doi:10.1177/0363546515585119. PMID 26116355. S2CID 26001387.
- ^ Braun C, McRobert CJ (May 2019). "Conservative management following closed reduction of traumatic anterior dislocation of the shoulder". The Cochrane Database of Systematic Reviews. 2019 (5): CD004962. doi:10.1002/14651858.CD004962.pub4. PMC 6510174. PMID 31074847.
- ^ Chalidis B, Sachinis N, Dimitriou C, Papadopoulos P, Samoladas E, Pournaras J (June 2007). "Has the management of shoulder dislocation changed over time?". International Orthopaedics. 31 (3): 385–9. doi:10.1007/s00264-006-0183-y. PMC 2267594. PMID 16909255.
- ^ Longo UG, Loppini M, Rizzello G, Ciuffreda M, Maffulli N, Denaro V (April 2014). "Management of primary acute anterior shoulder dislocation: systematic review and quantitative synthesis of the literature". Arthroscopy. 30 (4): 506–22. doi:10.1016/j.arthro.2014.01.003. PMID 24680311.
- ^ "Shoulder Scope". UW Orthopaedics and Sports Medicine, Seattle. 3 August 2012. Archived from the original on 13 October 2017. Retrieved 14 October 2017.
- ^ "Bankart repair for unstable dislocating shoulders". University of Washington: Orthopaedics and Sports Medicine. Archived from the original on 2008-01-15.
- ^ Burkhart SS, De Beer JF (October 2000). "Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion". Arthroscopy. 16 (7): 677–94. doi:10.1053/jars.2000.17715. PMID 11027751.
- ^ Burkhart SS, De Beer JF, Barth JR, Cresswell T, Criswell T, Roberts C, Richards DP (October 2007). "Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss". Arthroscopy. 23 (10): 1033–41. doi:10.1016/j.arthro.2007.08.009. PMID 17916467.
- ^ Noonan B, Hollister SJ, Sekiya JK, Bedi A (August 2014). "Comparison of reconstructive procedures for glenoid bone loss associated with recurrent anterior shoulder instability". Journal of Shoulder and Elbow Surgery. 23 (8): 1113–9. doi:10.1016/j.jse.2013.11.011. PMID 24561175.
- ^ a b Chen D, Goldberg J, Herald J, Critchley I, Barmare A (February 2016). "Effects of surgical management on multidirectional instability of the shoulder: a meta-analysis". Knee Surgery, Sports Traumatology, Arthroscopy. 24 (2): 630–9. doi:10.1007/s00167-015-3901-4. PMID 26658564. S2CID 35624937.
- ^ Millett PJ, Schoenahl JY, Register B, Gaskill TR, van Deurzen DF, Martetschläger F (February 2013). "Reconstruction of posterior glenoid deficiency using distal tibial osteoarticular allograft". Knee Surgery, Sports Traumatology, Arthroscopy. 21 (2): 445–9. doi:10.1007/s00167-012-2254-5. PMID 23114865. S2CID 8237748.
- ^ a b Fleega BA, El Shewy MT (May 2012). "Arthroscopic inferior capsular shift: long-term follow-up". The American Journal of Sports Medicine. 40 (5): 1126–32. doi:10.1177/0363546512438509. PMID 22437281. S2CID 11329565.
- ^ Mohtadi NG, Kirkley A, Hollinshead RM, McCormack R, MacDonald PB, Chan DS, et al. (August 2014). "Electrothermal arthroscopic capsulorrhaphy: old technology, new evidence. A multicenter randomized clinical trial". Journal of Shoulder and Elbow Surgery. 23 (8): 1171–80. doi:10.1016/j.jse.2014.02.022. PMID 24939380.
- ^ Kearney, Rebecca S.; Ellard, David R.; Parsons, Helen; Haque, Aminul; Mason, James; Nwankwo, Henry; Bradley, Helen; Drew, Stephen; Modi, Chetan; Bush, Howard; Torgerson, David; Underwood, Martin (2024-01-17). "Acute rehabilitation following traumatic anterior shoulder dislocation (ARTISAN): pragmatic, multicentre, randomised controlled trial". BMJ. 384: e076925. doi:10.1136/bmj-2023-076925. ISSN 1756-1833. PMC 10792684. PMID 38233068.
- ^ "Shoulder dislocation: a single physiotherapy session is usually sufficient". NIHR Evidence. 24 April 2024. doi:10.3310/nihrevidence_62848.
- ^ Wasserstein DN, Sheth U, Colbenson K, Henry PD, Chahal J, Dwyer T, Kuhn JE (December 2016). "The True Recurrence Rate and Factors Predicting Recurrent Instability After Nonsurgical Management of Traumatic Primary Anterior Shoulder Dislocation: A Systematic Review". Arthroscopy. 32 (12): 2616–2625. doi:10.1016/j.arthro.2016.05.039. PMID 27487737.